
November 2022 Health Care Polling Numbers
In November 2022, SecondStreet.org hired Leger to poll Canadians on health care. Here are the results …


In November 2022, SecondStreet.org hired Leger to poll Canadians on health care. Here are the results …
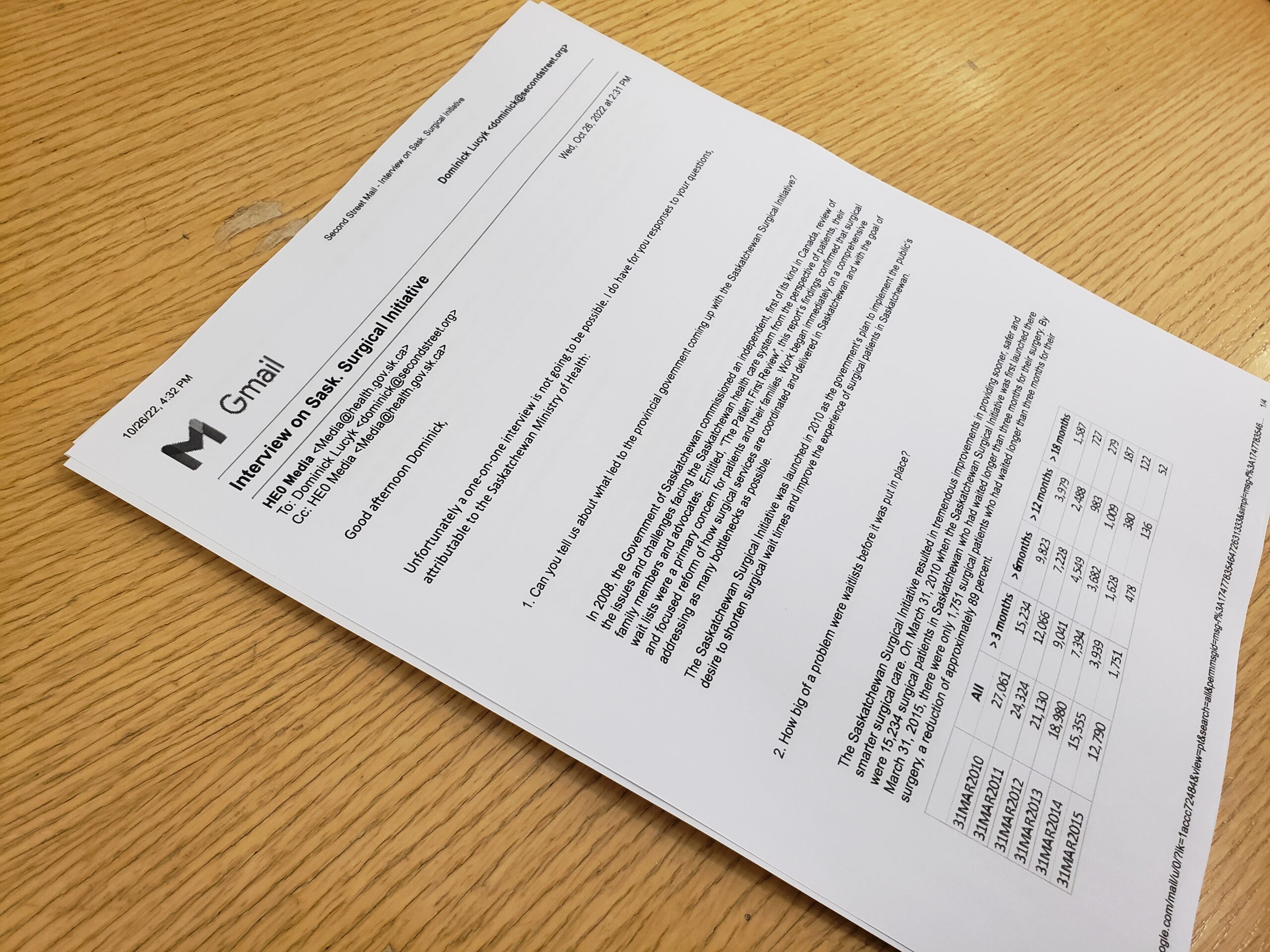
The prairie province launched its well-known “Saskatchewan Surgical Initiative” back in 2010 to reduce their waiting lists – some of the highest in the country at the time.
To learn more about this initiative we reached out to the Saskatchewan government for an interview.
They declined our request, but they did answer our questions in an email.

There’s been a lot of debate over the environmental impacts of different energy sources, and while competition between different types of energy is a good thing, it seems that some tend to get a free pass without much scrutiny.
Our Dom Lucyk goes over why wind power isn’t as consequence-free as many green activists say it is.

SecondStreet.org takes another look at the bill for Winnipeg’s city council pension plan.
SecondStreet.org recently wrote to Ontario’s Minister of Health to seek additional details on patients dying on waiting lists in the province.

SecondStreet.org continued our research into cool ways entrepreneurs are reducing emissions through new technology and processes.

Ukrainian Oksana Tkachuk breaks down ways that Canadians can support Ukraine during the ongoing invasion by Russian forces.
This 5-Point plan is taxpayer-friendly, helps reduce emissions, reduces global dependence on oil from dictatorships like Russia and creates private sector jobs without requiring subsidies.

We speak with Chris Vander Doelen from Harrow, Ontario about how his trip to Los Angeles saved his life from prostate cancer.

We sit down with Ken from Lillooet, British Columbia, to discuss how access to a private clinic saved his shoulder from irreparable damage.

Jim Carrey implied that Canada’s health care system was flawless, but does he know the facts about Canada’s growing waiting list crisis?

We discuss potential solutions for the hospital waiting list crisis, and what we as a country can do to fix our failing health care system.