



Over the past year, many provincial governments in Canada have been hiring private clinics to help address their surgical waiting list backlogs. A well-known example of where this approach was seen as a success is in the province of Saskatchewan. The prairie province launched its well-known “Saskatchewan Surgical Initiative” back in 2010 to reduce their waiting lists – some of the highest in the country at the time. To learn more about this initiative we reached out to the Saskatchewan government for an interview. While they declined our interview request, they did answer our questions in an email.
Can you tell us about what led to the provincial government coming up with the Saskatchewan Surgical Initiative?
In 2008, the Government of Saskatchewan commissioned an independent, first of its kind in Canada, review of the issues and challenges facing the Saskatchewan health care system from the perspective of patients, their family members and advocates. Entitled, “The Patient First Review”, this report’s findings confirmed that surgical wait lists were a primary concern for patients and their families. Work began immediately on a comprehensive and focused reform of how surgical services are coordinated and delivered in Saskatchewan and with the goal of addressing as many bottlenecks as possible.
The Saskatchewan Surgical Initiative was launched in 2010 as the government’s plan to implement the public’s desire to shorten surgical wait times and improve the experience of surgical patients in Saskatchewan.
How big of a problem were waitlists before it was put in place? The Saskatchewan Surgical Initiative resulted in tremendous improvements in providing sooner, safer and smarter surgical care. On March 31, 2010 when the Saskatchewan Surgical Initiative was first launched there were 15,234 surgical patients in Saskatchewan who had waited longer than three months for their surgery. By March 31, 2015, there were only 1,751 surgical patients who had waited longer than three months for their surgery, a reduction of approximately 89 percent. 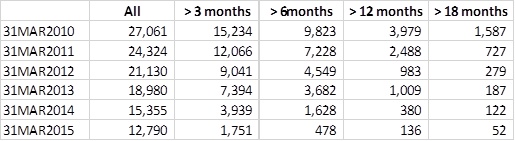 What led to the decision to partner up with private clinics to reduce the surgical backlog?
What led to the decision to partner up with private clinics to reduce the surgical backlog?
The first year goal of the Saskatchewan Surgical Initiative was to have no patients waiting longer than 18 months for surgery. The system was challenged to meet that goal and a year later, there remained more than seven hundred surgical patients still waiting 18 months for their surgeries.
It was decided that in addition to ramping up surgical capacity in publicly operated facilities, an expansion of publicly funded third-party delivery of selected surgical and diagnostic services should also be added to the Saskatchewan Surgical Initiative to further reduce wait times. Third-party facilities were contracted as a way to increase surgical volumes, without having patients jump the queue or pay for services.
Why not just hire more staff and do it internally?
Saskatchewan did hire more staff and increased surgical capacity in (its) publicly operated facilities. The Saskatchewan Surgical Initiative expanded both publicly and privately delivered surgical services to reduce wait times; however, additional capacity was required to address the backlog of those patients waiting longest.
Saskatchewan remains committed to publicly funded, publicly administered health care and maximizing surgical capacity in publicly operated facilities. By contracting third party facilities, this provided additional capacity for the Province to perform more surgeries in addition to those provided in hospital settings.
What were the results in terms of waiting list reductions? The Saskatchewan Surgical Initiative resulted in tremendous improvements in providing sooner, safer and smarter surgical care. On March 31, 2010 when the Saskatchewan Surgical Initiative was first launched there were 15,234 surgical patients in Saskatchewan who had waited longer than three months for their surgery. By March 31, 2015, there were only 1,751 surgical patients who had waited longer than three months for their surgery, a reduction of approximately 89 percent. 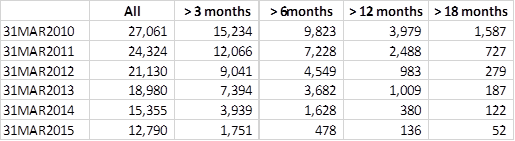 What about the cost? The Fraser Institute calculated a 26% cost savings versus doing the additional surgeries in-house. Is this similar to your own research?
What about the cost? The Fraser Institute calculated a 26% cost savings versus doing the additional surgeries in-house. Is this similar to your own research?
During the five years of the Surgical Initiative (2010-11 to 2014-15) the Government of Saskatchewan provided a cumulative investment was approximately $235M. The goal of this initiative was to remove bottlenecks in the surgical system and reduce wait times. Potential cost savings were not prioritized for consideration.
Costing comparisons of the original contract awards for third party surgical facilities demonstrated all procedures were performed below the cost of the public system. More recently, comparisons using estimated public system costing for surgeries based on a resource weight methodology developed by the Canadian Institute for Health Information show costs per procedure can vary based on complexity of the patient, we do not calculate actual cost per each procedure performed. Based on this more recent analysis, assessments showed that the difference between per-procedure costs in public hospitals and private surgical centres are roughly 35 per cent in plastic surgery and general surgery day procedures, and up to 45 per cent in orthopedic day procedures. Note that our private surgical partners typically perform less complex surgical cases as they are unable to keep a patient overnight or for an extended recovery, which contributes to some of the cost differences reported here.
How prevalent is the use of private clinics to this day in Saskatchewan? Publicly funded, privately delivered surgeries are not new to Saskatchewan as we have a long-standing and successful relationship with a third-party provider. Since 2010, more than 135,000 publicly funded surgeries have been performed by third party providers in Saskatchewan, roughly 15 per cent of the total number of surgeries completed in the province each year. In 2021-22, this increased to almost 20 per cent as they were able to increase their surgical volumes during the pandemic when the health system was faced with response to the pandemic that necessitated utilization of inpatient surgical beds to support COVID patients. Some critics say that private clinics are incentivized to cut corners. How do you make sure that private clinics stick to the same standards of care as government-run ones? Private third-party surgical providers enter into contracts with the Saskatchewan Health Authority requiring that they meet the required standards of care. They are also licensed and accredited by the College of Physicians and Surgeons of Saskatchewan which ensures the facility meets all requisite standards to provide quality and safe patient care. What’s your advice to other provincial governments that are considering the option of expanding or beginning to hire private clinics, as they deal with surgical backlogs? Surgical backlogs and wait lists are a primary concern for the public. Delays in surgeries can often result in poorer health outcomes. In our on-going work to reduce surgical wait times, the Government of Saskatchewan’s approach is to ensure that all the tools available are being utilized, both in public and privately operated facilities. This combination of increased surgical volumes in publicly operated facilities, as well as increased third party provision of surgical procedures, has proven successful in reducing overall wait times in Saskatchewan. The original email, provided by Dale Hunter with the Saskatchewan Ministry of Health, can be seen here.
Share on Facebook
Share on Twitter
You can help us continue to research and tell stories about this issue by making a donation or sharing this content with your friends. Be sure to sign up for our updates too!








