





Column
Share on twitter
Share on facebook
Share on linkedin
Share on email
New Canadian think tank SecondStreet.org released today a report that examines large cities in Canada and the double pensions they provide to some municipal employees. The study looked at 11 large cities: Vancouver, Edmonton, Calgary, Saskatoon, Winnipeg, Toronto, Ottawa, Mississauga, Brampton, Montreal and Halifax.
“Statistics Canada data shows most workers outside of government do not have a workplace pension, so it’s quite the perk for some city employees to receive two pensions upon retirement,” said SecondStreet.org President Colin Craig. “Municipalities that are looking to save taxpayers money could examine phasing out double pensions and just provide their basic pension, which is usually quite generous in its own right.”
Highlights from the report include:
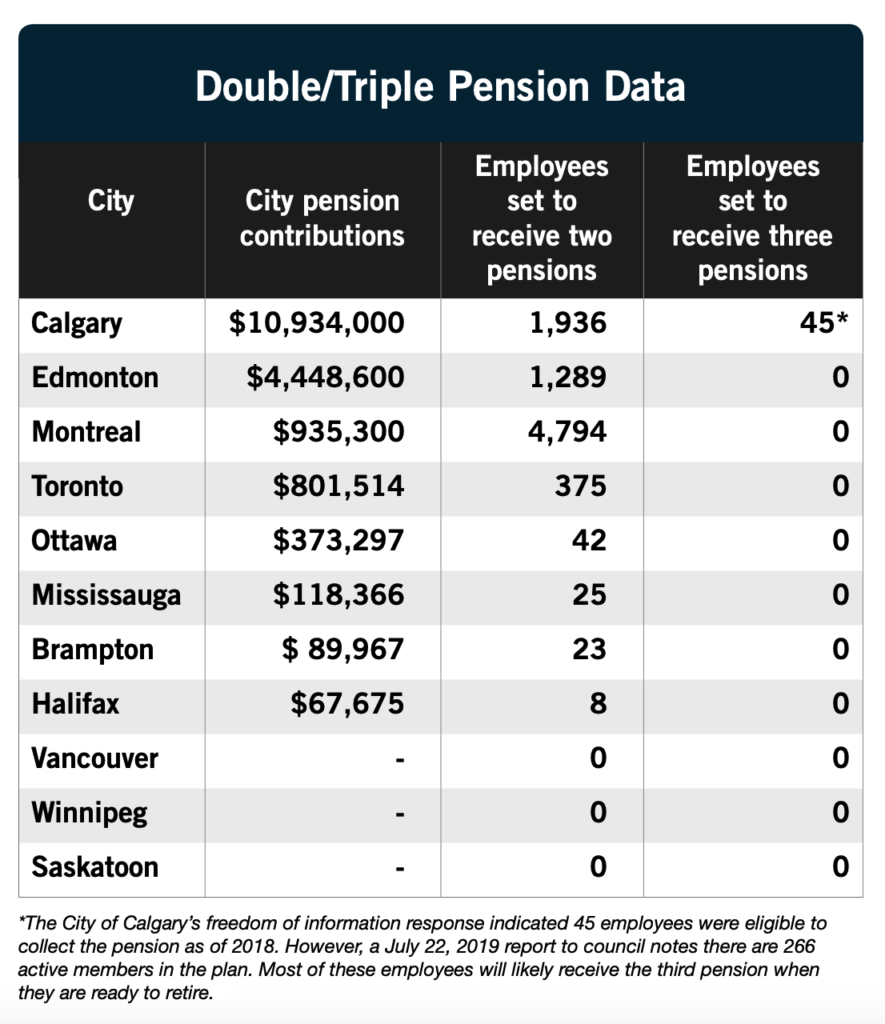
- Calgary spent $10.9 million on pension contributions for second and third pensions in 2018, more than the other ten cities combined. Edmonton spent the second highest amount at $4.4 million and Montreal was third at $0.9 million.
- Calgary was the only city to provide three pensions to some employees and it was 100% paid for by taxpayers (the bill for most pensions is split approximately 50/50).
- Halifax provided a secondary top-up pension to its top eight officials while Montreal, Calgary, Edmonton and Toronto provided the additional perk to hundreds, if not thousands, of employees.
- Vancouver, Winnipeg and Saskatoon indicated they do not provide secondary pensions to employees. (Saskatoon noted provincial legislation does not allow multiple pension situations.)
To view SecondStreet.org’s pension report – click here
To view responses from each city, see below:
Vancouver – click here
Edmonton – click here
Calgary – click here
Saskatoon – click here
Winnipeg – click here
Brampton – click here
Mississauga – click here
Toronto – click here
Ottawa – click here
Montreal – click here
Halifax – click here
Share on facebook
Share on Facebook
Share on twitter
Share on Twitter








