





Share on twitter
Share on facebook
Share on linkedin
Share on email
Jenny Mckenzie, Bruce MacDonald and countless others in Canada have been told they would have to wait years for surgery in the public health care system.
While their stories are anecdotes, we know they are putting real faces and names to a very large problem – a health care system that is struggling with long waiting lists.
And when government programs struggle, some politicians and special interest groups inevitably suggest the solution is simply for the government to spend even more money.
But is that really the answer to our health care system’s woes?
No.
Consider a few big picture numbers from British Columbia.
In 2019, the B.C. Anesthesiologists’ Society released a report with figures on B.C.’s population and waiting list data:
Population:
2001/02 – 4,100,000
2017/18 – 4,800,000 (up 18.2%)
Patients waiting for surgery:
2001/02 – 55,367
2017/18 – 85,468 (up 54.4%)
In short, the province’s population is up a bit, yet waiting lists have grown more than twice as fast. With these figures in mind, we looked at government spending in B.C. on health care.
If we are to believe an increase in spending will increase services then surely the decrease in service levels can be explained by a decrease in spending … right?
That’s not the case.
If you look at “Table F” from the Canadian Institute for Health Information, you’ll find spending exploded during the same period:
B.C. government health care spending:
2001/02 – $10.380 billion
2017/18 – $20.255 billion (up 95%)
B.C. government per capita health care spending:
2001/02 – $2,537.42
2017/18 – $4,183.96 (up 65%)
According to the Bank of Canada’s inflation calculator, Canada’s inflation rate was about 34% during this period. B.C.’s inflation rate may differ a bit, but inflation is not likely to be the culprit of growing waiting lists.
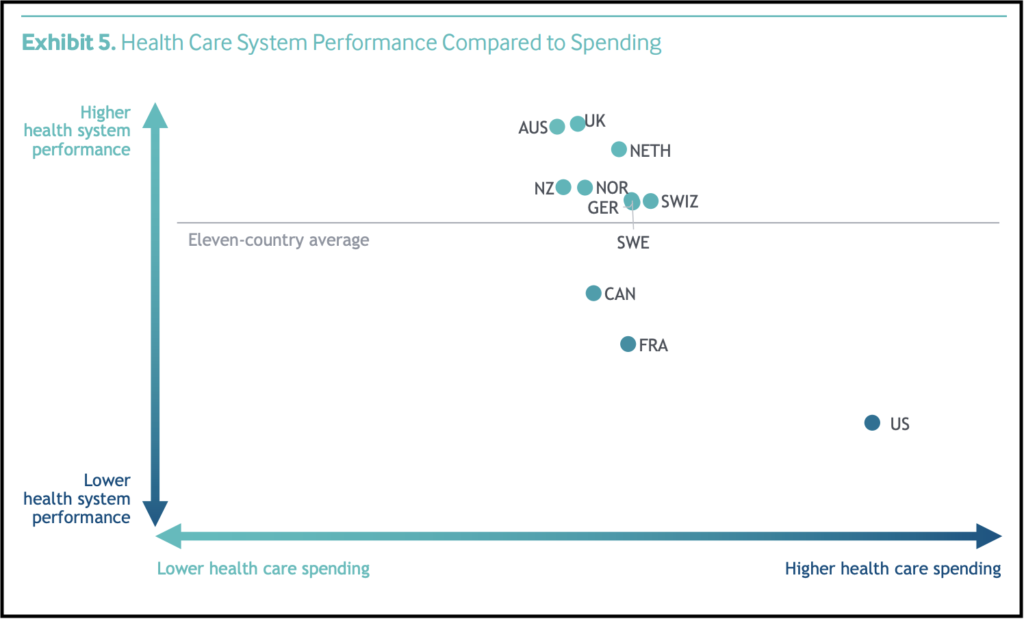
If we compare Canada’s health care system with other nations, the data suggests we’re just not getting very good bang for our buck.
This 2017 report (click here) from the progressive Commonwealth Fund shows that Norway, the United Kingdom, Australia and New Zealand are all performing much better than Canada, while spending less. See this chart from the report:
This obviously brings us to the question of – what do we need to do to improve outcomes for patients?
As we noted in our recent policy brief The flight of the sick, we sat down with the Fraser institute’s Bacchus Barrua to discuss health care reform and what needs to be done.
Barrua described three common features among countries that are achieving better results with their universal health care systems (Germany, Switzerland, France, the Netherlands, Australia, Sweden):
- They have a different attitude towards the private sector – Rather than seeing the private sector as the enemy, they see the private sector as a partner to help deliver services. (Including as a pressure valve that helps reduce demand on the public system).
- Patients share in the cost of treatment – Patients are required to contribute to the cost of services in an affordable manner (with limits to ensure no one has to choose between health care and their mortgage). This approach helps ensure patients think of health care as a service that should be used wisely.
- These countries fund their hospitals differently – Most hospitals in Canada are funded through a “global budget” that is set at the beginning of the year and then spent. More effective health care models fund hospitals based on productivity so there is an incentive to provide better, higher quality care with better results for patients.
Colin Craig is the President of SecondStreet.org
Share on facebook
Share on Facebook
Share on twitter
Share on Twitter
Other Canadians Share Similar Experiences:
Play Video
Don and Jackie, Winnipeg
Play Video
Jerry and Becky, Calgary
Play Video
Troy and Erika, Victoria
Play Video
Jim Jones, Toronto
You can help us continue to research and tell stories about this issue by making a donation
or sharing this content with your friends. Be sure to sign up for our updates too!








