




Share on twitter
Share on facebook
Share on linkedin
Share on email
Several years ago a contact from Winnipeg told me about how he once drove to Minnesota to get an MRI for his shoulder.
Manitoba’s government-run health care system had told Ken that he would have to wait a year or so for the procedure. He found that to be unacceptable. The guy was pretty active – liked to play sports, had kids who were still at home – he didn’t want to sit on the sidelines for a year.
At the same time, the Manitoba government had essentially outlawed private clinics from selling MRI scans to the public. That made Ken’s choice clear – wait for a year in discomfort or leave the province and pay out-of-pocket for faster care.
Ken drove to Minnesota paid around $800 for an MRI scan and if I remember correctly, he stayed a few extra days to do some shopping.
His experience, and others like it, has always struck me as strange. By limiting private health care options in the province, the Manitoba government pushed economic activity outside of its borders.
The $800 Ken spent in Minnesota supported jobs in Minnesota and the American company that provided the service – both of which would in turn pay taxes to the U.S. government (which could be used to fund the U.S. health care system).
But it wasn’t just the $800 cost for the procedure that would help the U.S. economy, Ken also spent money on fuel for his car, a hotel, food and shopping. All those dollars could have stayed in Manitoba had the province relaxed its regulations around what it allows private clinics to offer.
With stories like Ken’s in mind, I decided to do some digging into medical tourism. Here are a couple interesting tidbits that I came across:
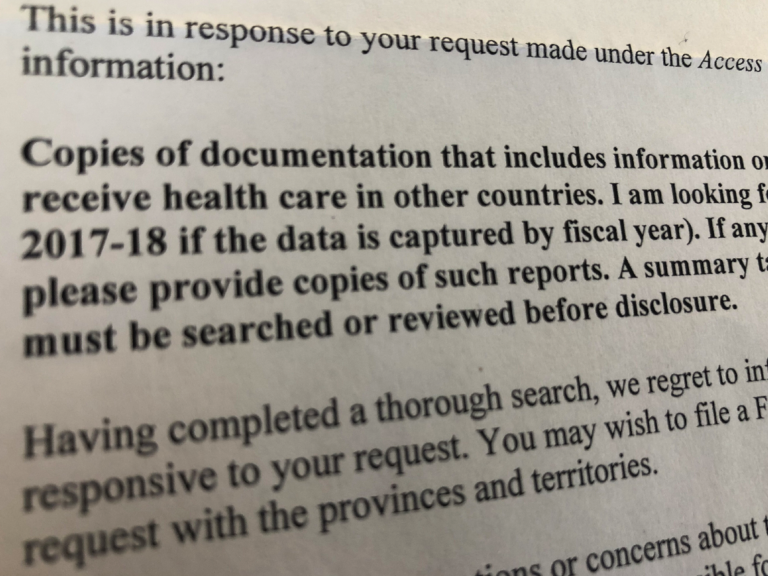
1) In September 2018, I asked the government of Canada about cases like Ken’s – how many Canadians leave the country each year for health care? As the federal government provides provincial governments with billions of dollars each year in health care funding, I thought Ottawa might also track how many Canadians were dissatisfied with the service so much that they left the country.
Health Canada responded that it has no information on the situation. You can see their response if you click here.
2) While health care delivery is a provincial responsibility, the federal government’s Department of Health sometimes flexes its muscles in this area by financially penalizing (or threatening to penalize) provincial governments when they experiment with various forms of private health care. (See this story about Saskatchewan, this one about Ontario and this one about British Columbia.)
With those stories in mind, it was interesting to see the federal government’s Department of Innovation Science and Economic Development recognize the “success story” of a private health care entrepreneur.
On the federal government’s website you’ll find the story of Adele Kulyk, an entrepreneur from Saskatchewan who runs Global Healthcare Connections Inc., a medical tourism company that helps connect Canadians with health care services in other countries – hip operations, cancer procedures, bariatric surgery, etc.
No disrespect to Ms. Kulyk. If you look at her company’s website, you’ll see she has helped improve the health and well-being of many patients.
But when it comes to the idea of allowing Canadians more choice in health care, the contrast between Ottawa’s two departments is quite striking.
Colin Craig is the President of SecondStreet.org
Share on facebook
Share on Facebook
Share on twitter
Share on Twitter
Other Canadians Share Similar Experiences:
Play Video
Don and Jackie, Winnipeg
Play Video
Jerry and Becky, Calgary
Play Video
Troy and Erika, Victoria
Play Video
Jim Jones, Toronto
You can help us continue to research and tell stories about this issue by making a donation
or sharing this content with your friends. Be sure to sign up for our updates too!








